



Avoid costly audit findings with MedDRA Coding in Clinical Trials best practices that improve compliance, safety data accuracy, and regulatory readiness
The Importance of MedDRA Coding
In the high-stakes world of clinical trials, accurate adverse event reporting isn’t just a regulatory checkbox, it’s the foundation of patient safety, data integrity, and successful regulatory submissions. MedDRA (Medical Dictionary for Regulatory Activities) serves as the global standard for coding medical terms, transforming messy verbatim reports from investigators into structured, analyzable data that regulators like the FDA and EMA can trust.Poor coding can lead to signal detection failures, delayed approvals, or audit findings that derail entire programs. Yet, when done right with robust processes, it ensures audit readiness and builds confidence in your safety database.
Understanding the MedDRA Hierarchy
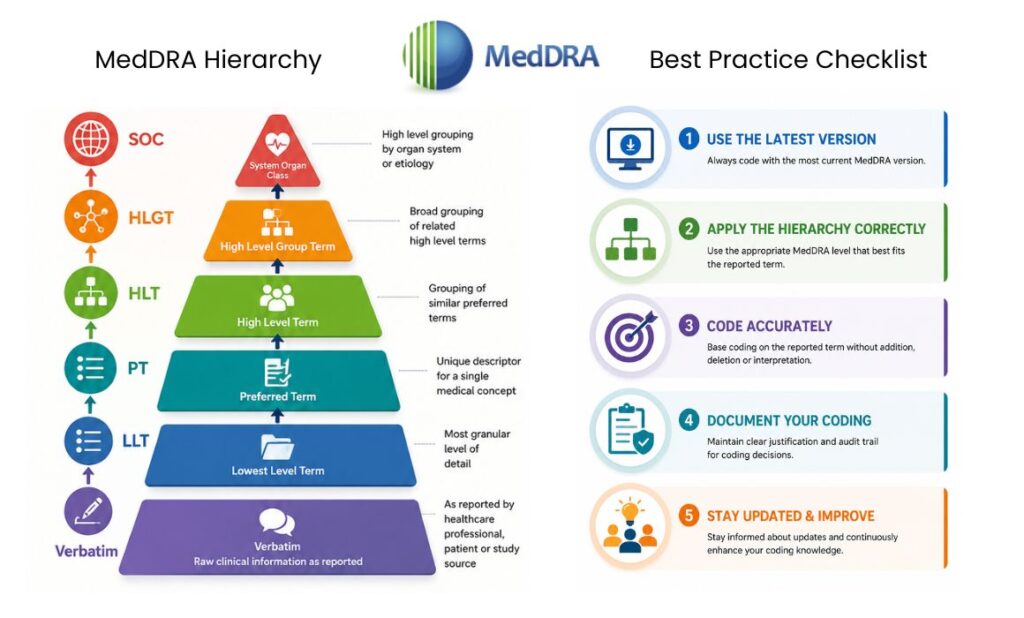
MedDRA’s multi-axial, hierarchical structure is what makes it powerful, and sometimes challenging. It organizes terms across five levels:
- Lowest Level Terms (LLTs): Most specific, often match verbatim reports.
- Preferred Terms (PTs): The primary level for analysis and reporting.
- High Level Terms (HLTs).
- High Level Group Terms (HLGTs).
- System Organ Classes (SOCs): Broadest categories (e.g., Cardiac disorders, Nervous system disorders).
This structure allows granular coding while enabling meaningful aggregation for safety reviews. Always select the most appropriate current LLT, which automatically links to its PT and higher levels.
Mastering this hierarchy is key to consistency, especially in global trials where investigators from different backgrounds report events variably.
Core Best Practices for Accurate MedDRA Coding
Start Strong: Quality Source Data and Training
The foundation of excellent coding is excellent source data. Clear, concise verbatim terms from CRFs reduce ambiguity. Train investigators on precise reporting, avoid abbreviations, jargon, or vague descriptions like “felt bad.”Coders themselves need rigorous training. Certified or experienced medical coders familiar with ICH guidelines perform better. Organizations should maintain detailed coding conventions documents covering misspellings, abbreviations, combination terms, and “always query” scenarios (e.g., “chest pain”).
Follow ICH Points to Consider
The official MedDRA Term Selection: Points to Consider (updated annually) is your bible. Key principles include:
- Do not alter MedDRA terms.
- Select only current LLTs.
- Use medical judgment without adding or interpreting information beyond the verbatim.
- Code all reported concepts without over-coding.
Consistency across coders is critical. Regular calibration sessions and dual-review for complex cases help minimize variability, which studies show can affect 10-12% of terms otherwise.
Implement Robust Quality Assurance Processes
Audit readiness starts with proactive QA:
- Automated coding tools supplemented by manual review.
- Peer review or second-level coding for serious adverse events (SAEs).
- Regular quality metrics tracking (e.g., coding disagreement rates).
- Reconciliation processes between safety and clinical databases.
Document everything, coding decisions, queries to sites, and rationales, for traceability during audits.
Version Management: Navigating Updates Without Disruption
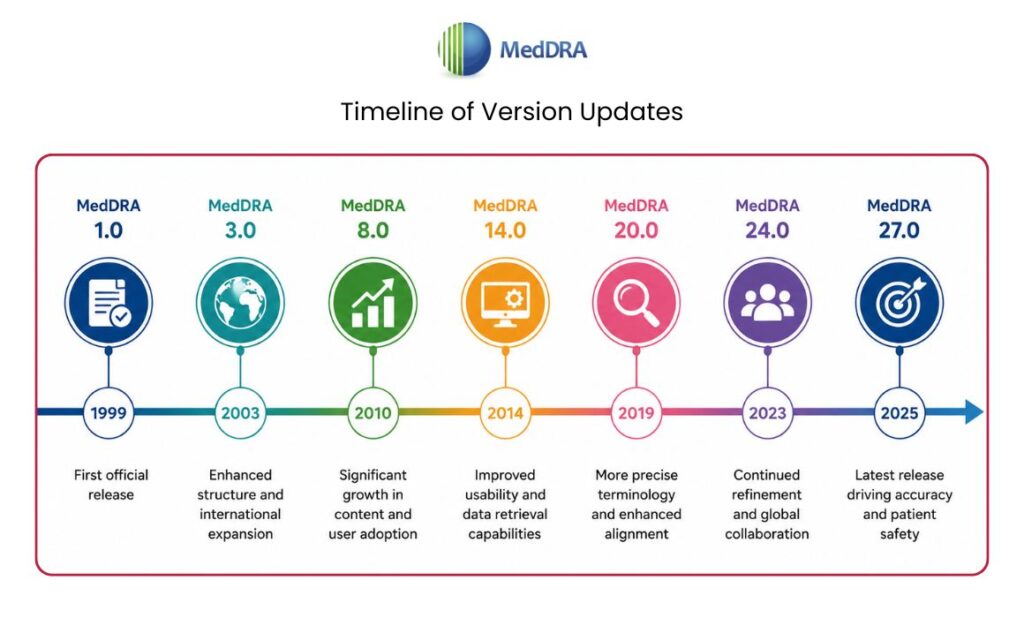
MedDRA releases updates twice yearly (March and September). For long-running trials, frequent recoding isn’t practical. The MSSO recommends practical options like freezing a version at study start and optionally recoding at major milestones (e.g., database lock or ISS preparation). Many adopt a strategy of using the latest version at the beginning and recoding the full project dataset periodically.
Table: MedDRA Versioning Options for Clinical Trials
| Option | Description | Pros | Cons | Best For |
| 1. Freeze at start, use throughout | Lock version for entire project | Simplicity, consistency | Misses new terms | Short trials |
| 2-4. Various milestone updates | Selective recoding | Balanced | Resource intensive | Mid-size programs |
| 5-6 (Recommended) | Freeze per trial; recode project at key points or ongoing with latest | Regulatory alignment, signal detection | Requires planning | Large/global programs with ISS needs |
Choose based on trial duration, regulatory strategy, and resources. Tools like the MedDRA Version Analysis Tool (MVAT) aid transitions.
Common Pitfalls and How to Avoid Them
Even experienced teams stumble on:
- Ambiguous verbatims: “Pain in leg” – query for specificity rather than guessing.
- Combination terms: Code components separately if needed (e.g., “nausea and vomiting”).
- Over- or under-coding: Stick strictly to reported information.
- Inconsistent handling of “due to” phrases or linked events.
- Ignoring hierarchy checks: Always verify the PT and SOC placement.
Proactive query management with sites and clear conventions prevent these issues. Regular internal audits simulate regulatory scrutiny.
Technology’s Role in Modern MedDRA Coding
Auto-coders and AI-assisted tools speed up the process while maintaining accuracy when paired with expert oversight. Integrated EDC systems with MedDRA dictionaries enable real-time coding support. However, technology doesn’t replace human judgment for nuanced cases.For organizations handling multiple trials, centralized coding teams or specialized medical coding services ensure consistency and free up internal resources for core trial activities. Similarly, expert pharmacovigilance support can strengthen overall safety monitoring and audit preparation.
Ensuring Audit Readiness: From Coding to Submission
Auditors scrutinize coding consistency, documentation, and process adherence. Be ready with:
- Complete audit trails.
- Version control records.
- Training documentation.
- Quality control reports.
- Justification for coding decisions.
Mock audits and gap analyses keep teams sharp. Integrate coding best practices into your overall data management and quality systems from study startup.
The Payoff: Better Safety Signals and Smoother Approvals
Effective MedDRA coding doesn’t just satisfy regulators, it uncovers true safety profiles faster, protects participants, and accelerates development timelines. In an era of increasing trial complexity and scrutiny, investing in coding excellence pays dividends.By partnering with experienced providers for data management solutions or clinical safety services, sponsors can maintain focus on innovation while upholding the highest standards of data quality.
Read More : Understanding 2025 Global Clinical Trial Compliances for CRO Operational Excellence
References
- MedDRA Official Website – https://www.meddra.org/
- ICH MedDRA Term Selection: Points to Consider – Available via MedDRA resources.
- MSSO Best Practices for MedDRA Maintenance and Versioning in Clinical Trials – MedDRA Best Practice Document.
- Advarra: Standardization and Medical Coding Dictionaries – https://www.advarra.com/blog/standardization-and-the-importance-of-medical-coding-dictionaries-in-clinical-trials/.
FAQs on MedDRA Coding in Clinical Trials
When should MedDRA coding begin in a clinical trial?
Ideally at study startup with dictionary integration into CRFs and EDC. Early coding during data collection minimizes downstream rework.
Can I change the MedDRA version mid-trial?
It’s generally discouraged to avoid inconsistencies, but possible at predefined milestones with full recoding and documentation. Plan versioning strategy upfront.
Who should perform MedDRA coding—site staff or central team?
Central experienced coders or specialists are preferred for consistency. Site staff should focus on accurate verbatim reporting.
How do I handle discrepancies between coders?
Establish adjudication processes, use calibration exercises, and document resolutions. Aim for measurable quality targets.
What role do SMQs play in MedDRA coding?
Standardised MedDRA Queries (SMQs) are retrieval tools for signal detection, not for initial coding. They help analyze coded data effectively.
